- Developmental Dysplasia of the Hip is a disorder of abnormal development of the hip secondary to capsular laxity and mechanical instability.
- DDH encompasses a spectrum of disease that includes
- dysplasia
- shallow or underdeveloped acetabulum
- subluxation
- displacement of the joint with some contact remaining between the articular surfaces
- dislocation
- complete displacement of the joint with no contact between the original articular surfaces
- dysplasia
- Epidemiology
- Incidence
- most common hip orthopaedic disorder in newborns
- dysplasia is 1:100
- dislocation is 1:1000
- Demographics
- more common infemales (6:1)
- Anatomic location
- most common inleft hip (60%)
- due to the most common intrauterine position being left occiput anterior (left hip is adducted against the mother’s lumbrosacral spine)
- bilateral in 20%
- most common inleft hip (60%)
- Risk factors
- firstborn
- due to unstretched uterus and tight abdominal structures compressing the uterus
- female
- due to increased ligamentous laxity that transiently exists as the result of circulating maternal hormones and the estrogens produced by the fetal uterus
- breech
- more commonly seen in female children, firstborn children, and pregnancies complicated by oligohydramnios
- higher risk of DDH with frank/single breech position compared to footling breech position
- family history
- oligohydramnios
- macrosomia
- limited hip abduction
- talipes
- swaddling
- firstborn
- Pathophysiology
- etiology
- initial instability thought to be caused by maternal and fetal laxity, genetic laxity, and intrauterine and postnatal malpositioning
- pathoanatomy
- initial instability leads to dysplasia
- typical deficiency is anterior or anterolateral acetabulum
- dysplasia leads to subluxation and gradual dislocation
- repetitive subluixation of the femoral head leads to the formation of a ridge of thickened articular cartilage called thelimbus
- chronic dislocation leads to
- development of secondary barriers to reduction
- pulvinar thickens
- ligamentum teres thickens and elongates
- transverse acetabular ligament hypertrophies
- hip capsule and iliopsoas form hourgass configuration
- anatomic changes
- increased femoral anteversion
- flattening of the femoral head
- increased acetabular anteversion
- increased obliquity and decreased concavity of the acetabular roof
- thickening of the medial acetabular wall
- Associated conditions
- congenital muscular torticollis(20%)
- metatarsus adductus(10%)
- congenital knee dislocation
- conditions characterized by increased amounts of type III collagen
- development of secondary barriers to reduction
- Presentation
- Physical exam (< 3 months)
- mainstay of physical diagnosis is palpable hip subluxation/dislocation on exam
- Barlow
- dislocates adislocatable hip by adduction and depression of the flexed femur
- “click of exit”
- Ortolani
- reduces adislocated hip by elevation and abduction of the flexed femur
- “click of entry”
- Galeazzi (Allis)
- apparent limb length discrepancy due to aunilateral dislocated hip with hip flexed at 90 degrees and feet on the table
- femur appears shortened on dislocated side
- Barlow and Ortolani are rarely positive after 3 months of age because of soft-tissue contractures that form around the hip
- Barlow
- Physical exam (> 3 months to 1 year)
- limitations in hip abduction
- most sensitive test once contractures have begun to occur
- occurs as laxity resolves and stiffness begins to occur
- decreased symmetrically in bilateral dislocations
- leg length discrepancy predominates
- Klisic test
- used to detect bilateral dislocations
- line from the long finger placed over the greater trochanter and the index finger over the ASIS should point to the umbilicus
- if the hip is dislocated, the line will point halfway between the umbilicus and pubis
- Physical exam (> 1 year – walking child)
- pelvic obliquity
- lumbar lordosis
- in response to hip contractures resulting from bilateral dislocations in a child of walking age
- Trendelenburg gait
- results from abductor insufficiency
- toe-walking
- attempt to compensate for the relative shortening of the affected side
- Imaging
- Radiograph
- indications
- recommended views
- AP of pelvis
- measurements
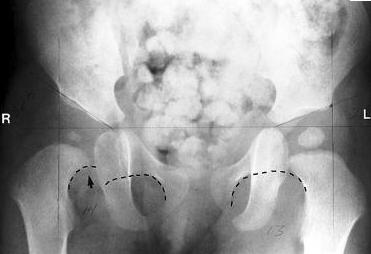
- hip dislocation
- Hilgenreiner’s line
- horizontal line through the right and left triradiate cartilage
- femoral head ossification should beinferior to this line
- Perkin’s line
- line perpendicular to Hilgenreiner’s line through a point at the lateral margin of the acetabulum
- femoral head ossification should bemedial to this line
- Shenton’s line
- arc along the inferior border of the femoral neck and the superior margin of the obturator foramen
- arc line should becontinuous
- delayed ossification of the femoral head is seen in cases of dislocation
- acetabular teardrop not typically present prior to hip reduction for chronic dislocations since birth
- development of teardrop after reduction is thought to be a good prognostic sign for hip function
- hip dysplasia
- acetabular index (AI)
- center-edge angle (CEA) of Wiberg
- angle formed by Perkin’s line and a line from the center of the femoral head to the lateral edge of the acetabulum
- < 20° is considered abnormal
- only reliable in patients > 5 years old
- Ultrasound
- indications
- primary imaging modality from birth to 4 months
- may produce spurious results if performed before 4-6 weeks of age
- positive physical exam
- risk factors (family history or breech presentation)
- AAP recommends an US study at 6 weeks in patients who are considered high risk (family history or breech presentation) despite normal exam
- monitoring of reductionduring Pavlik harness treatment
- most studies show it is not cost effective for routine screening
- primary imaging modality from birth to 4 months
- findings
- measurements
- staging
- Graf classification
- Screening
- All infants require screening
- physical exam
- successful screening requires repetitive screening until walking age
- ultrasound
- ultrasound screening of all infants occurs in many countries; however, it has not been proven to be cost-effective
- recommendation is to perform ultrasound at 4-6 weeks in patients with
- risk factors
- positive physical findings
- Treatment in children
- Non-operative
- Pavlik harness
- indications
- < 6 months old andreducible hip
- contraindicated in teratologic hip dislocations and patients with spina bifida or spasticity
- requires normal muscle function for successful outcomes
- closed reduction and spica casting
- indications
- 6-18 months old
- failure of Pavlik treatment
- Operative
- open reduction and spica casting
- indications
- > 18 months old
- failure of closed reduction
- open reduction and femoral osteotomy
- indications
- > 2 years old with residual hip dysplasia
- anatomic changes on femoral side (e.g., femoral anteversion, coxa valga)
- best in younger children (< 4 years old)
- after 4 years old, pelvic osteotomies are utilized
- open reduction and pelvic osteotomy
- indications
- > 2 years old with residual hip dysplasia
- severe dysplasia accompanied by significant radiographic changes on the acetabular side (increased acetabular index)
- used more commonly in older children (> 4 yr)
- decreased potential for acetabular remodeling as child ages
- Complications
- AVN
- seen with all forms of treatment
- increased rates associated with
- excessive orforceful abduction
- previousfailed closed treatment
- repeat surgery
- diagnosis based on radiographic findings that include
- failure of appearance or growth of the ossific nucleus 1 year after the reduction
- broadening of the femoral neck
- increased density and fragmentation of ossified femoral head
- residual deformity of proximal femur after ossification
- Delayed diagnosis
- bilateral dislocations
- patients typically function better if hips are not reduced if 6 years of age or older
- unilateral dislocation
- better outcomes without surgical treatment if the patient is > 8 years old
- epiphysiodesis can be performed for treatment of limb length discrepancy
- Recurrence
- approximately 10% with appropriate treatment
- requires radiographic follow-up until skeletal maturity
- bilateral dislocations
- AVN
- indications
- indications
- indications
- open reduction and spica casting
- indications
- indications
- Pavlik harness
- Non-operative
- physical exam
- All infants require screening
- indications
- Hilgenreiner’s line
- hip dislocation
- Radiograph
- limitations in hip abduction
- mainstay of physical diagnosis is palpable hip subluxation/dislocation on exam
- Physical exam (< 3 months)
- initial instability leads to dysplasia
- etiology
- Incidence




{kind=link}
{kind=link}
{kind=link}
{kind=link}